 Contact A Representative Since 1963, Cook Medical has been a champion of minimally invasive treatment options for patients. In the case of the centesis and drainage procedural areas, the healthcare industry discussion has largely centered around the efficacy of large-bore… Contact A Representative Since 1963, Cook Medical has been a champion of minimally invasive treatment options for patients. In the case of the centesis and drainage procedural areas, the healthcare industry discussion has largely centered around the efficacy of large-bore…
Contact A Representative Since 1963, Cook Medical has been a champion of minimally invasive treatment options for patients. In the case of the centesis and drainage procedural areas, the healthcare industry discussion has largely centered around the efficacy of large-bore… Contact A Representative Since 1963, Cook Medical has been a champion of minimally invasive treatment options for patients. In the case of the centesis and drainage procedural areas, the healthcare industry discussion has largely centered around the efficacy of large-bore…  Contact A Representative We offer an extensive line of chest tubes for removing both air and fluid from the pleural and pericardial spaces. These products are available in a variety of designs and sizes, including several small-bore configurations, Seldinger and…
Contact A Representative We offer an extensive line of chest tubes for removing both air and fluid from the pleural and pericardial spaces. These products are available in a variety of designs and sizes, including several small-bore configurations, Seldinger and…  Lung ultrasound is a necessary, key component in both pulmonary and critical care settings due to its high diagnostic accuracy and physicians’ ability to perform it at the bedside. In cases of pleural disease, lung ultrasound could be an essential…
Lung ultrasound is a necessary, key component in both pulmonary and critical care settings due to its high diagnostic accuracy and physicians’ ability to perform it at the bedside. In cases of pleural disease, lung ultrasound could be an essential…  Dr. Nichole Tanner discusses how to optimize tissue acquisition during EBUS procedures Nichole Tanner, MD, MSCR, discussed how to optimize tissue acquisition during endobronchial ultrasound (EBUS) procedures at a lecture during American Thoracic Society International Conference. Currently, Dr. Tanner is…
Dr. Nichole Tanner discusses how to optimize tissue acquisition during EBUS procedures Nichole Tanner, MD, MSCR, discussed how to optimize tissue acquisition during endobronchial ultrasound (EBUS) procedures at a lecture during American Thoracic Society International Conference. Currently, Dr. Tanner is…  Dr. Pasquale “Pat” Ciaglia became a physician inventor late in his career. However, this late start didn’t stop him from developing several important products to improve patient care. The most notable one was the Ciaglia Blue Rhino® Percutaneous Tracheostomy Introducer in…
Dr. Pasquale “Pat” Ciaglia became a physician inventor late in his career. However, this late start didn’t stop him from developing several important products to improve patient care. The most notable one was the Ciaglia Blue Rhino® Percutaneous Tracheostomy Introducer in…  Tim Buchman, PhD, MD, is the current editor-in-chief of Critical Care Medicine (CCM), a peer-reviewed, publication leader in critical care medicine. CCM covers all specialties for acute and emergency care, such as chest physicians, surgeons, pediatricians, pharmacists/pharmacologists, anesthesiologists, and critical…
Tim Buchman, PhD, MD, is the current editor-in-chief of Critical Care Medicine (CCM), a peer-reviewed, publication leader in critical care medicine. CCM covers all specialties for acute and emergency care, such as chest physicians, surgeons, pediatricians, pharmacists/pharmacologists, anesthesiologists, and critical…  At Cook, we were among the first to recognize the clinical impact of EBUS procedures. That’s why we focused our expertise as market leaders in ultrasound needles to create a full range of EchoTip® EBUS needles to meet your sampling needs.…
At Cook, we were among the first to recognize the clinical impact of EBUS procedures. That’s why we focused our expertise as market leaders in ultrasound needles to create a full range of EchoTip® EBUS needles to meet your sampling needs.… 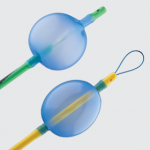 Our endobronchial blocker allows one-lung ventilation through a conventional single-lumen endotracheal tube that is easier to place and poses a lower risk of trauma to internal structures than a double-lumen tube.1 View the Arndt Endobronchial Blocker’s indications for use, specifications,…
Our endobronchial blocker allows one-lung ventilation through a conventional single-lumen endotracheal tube that is easier to place and poses a lower risk of trauma to internal structures than a double-lumen tube.1 View the Arndt Endobronchial Blocker’s indications for use, specifications,…  Now you can explore our complete line of difficult airway products all in one place. On this mobile-friendly site, you can discover how our products facilitate successful intubation, airway exchange, and emergency airway access. Intubation Our intubating introducers allow you to provide oxygen…
Now you can explore our complete line of difficult airway products all in one place. On this mobile-friendly site, you can discover how our products facilitate successful intubation, airway exchange, and emergency airway access. Intubation Our intubating introducers allow you to provide oxygen…  Professor Giulio Frova offers insight into the world of anesthesiology, how he came up with the idea for the Frova Intubating Introducer, and how to handle difficult intubations. What inspired you to pursue a career in anesthesiology? It was a…
Professor Giulio Frova offers insight into the world of anesthesiology, how he came up with the idea for the Frova Intubating Introducer, and how to handle difficult intubations. What inspired you to pursue a career in anesthesiology? It was a…  Early mobility has become an increasingly important topic in critical care medicine. To help spread the word on this key issue, we talked to Dr. Paul Marik and Dr. Bruce Friedman, two intensivists at the forefront of this topic. Why…
Early mobility has become an increasingly important topic in critical care medicine. To help spread the word on this key issue, we talked to Dr. Paul Marik and Dr. Bruce Friedman, two intensivists at the forefront of this topic. Why…  In this video, airway management pioneer Professor Peter Charters begins his presentation at the World Airway Management Meeting (WAMM) in Dublin with a demonstration of the Aintree Intubation Catheter for a laryngeal mask airway exchange. Professor Charters then explains multiple difficult laryngeal…
In this video, airway management pioneer Professor Peter Charters begins his presentation at the World Airway Management Meeting (WAMM) in Dublin with a demonstration of the Aintree Intubation Catheter for a laryngeal mask airway exchange. Professor Charters then explains multiple difficult laryngeal…  As we look back on our history with Dr. Pat Ciaglia, we talked to Staffan Grigholm, a retired employee who was one of our company's original seven sales representatives. Staffan (in plaid pants) made the initial contact between Cook and Dr.…
As we look back on our history with Dr. Pat Ciaglia, we talked to Staffan Grigholm, a retired employee who was one of our company's original seven sales representatives. Staffan (in plaid pants) made the initial contact between Cook and Dr.…