Contributed by Dr. M. Fuad Azrak

M. Fuad Azrak
MD, MPH
Beaumont Health
Wayne, MI
Presentation and diagnosis
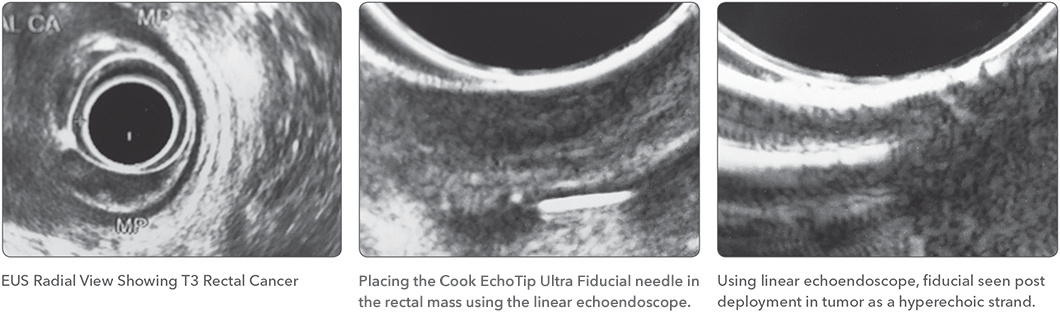
A 57-year-old patient was recently diagnosed with rectal adenocarcinoma and was referred for rectal ultrasound for staging. Fiducial markers placement was requested by radiation oncology if the patient has locally advanced disease. The initial examination was done using a radial echoendoscope. The patient had a semi-circumferential mass that disrupted the muscularis propria but did not invade other adjacent structures. The patient was staged as T3N0MX.
Procedure
A 22-gauge Cook EchoTip Ultra Fiducial needle was placed in the linear echoendoscope. This needle is preloaded with 4 fiducials. The echoendoscope was passed into the rectum beyond the mass. The upper edge of the mass was identified by the sudden mucosal thickening. The needle was deployed into the upper margin of the tumor mass under ultrasound guidance and then slightly retracted to create a small track. The fiducial was deployed by advancing the stylet forward and was visible as a hyperechoic strand.
The EchoTip Ultra Fiducial Needle was retracted into the scope and the echoendoscope was rotated slowly until the first fiducial marker disappeared from view then another fiducial was deployed in the same position. The echoendoscope was then pulled until the lower margin of the tumor was identified by the visual and ultrasound views.
Outcome
Two more fiducials were deployed in the same fashion under ultrasound guidance. All four markers were deployed around tumor margins.
This technique enables the dispersed placement of the markers rather than having all markers concentrated in one place within the tumor. Fluoroscopic guidance could be also used to confirm the dispersed placement of markers.
Dr. M. Fuad Azrak is a clinical assistant professor at Wayne State University School of Medicine in Detroit, Michigan and chairs the Endoscopy Committee of Beaumont Hospital, Wayne, Michigan.
Dr. M. Fuad Azrak is not a paid consultant of Cook Medical.