In 2019, a retrospective study by Diaz, et al1, compiled and analyzed data from 50,545 lead extraction cases from 2011-2016. The authors compared mortality rates for laser sheaths and rotational sheaths. A retrospective analysis comparing these two treatment modalities had never before been conducted.
Using device procedure data provided by a third party, the authors estimated that physicians performing lead extractions chose laser sheaths for 64% of procedures, compared to using rotational sheaths 36% of the time.
The study showed that lead extraction with laser sheaths appears to be associated with a higher risk of mortality when compared to rotating sheaths. Patients treated with laser sheaths had a mortality rate 7.2 times greater than those whose leads were extracted using rotational sheaths. The authors called for further studies to confirm the results1.
History of Lead Extraction Devices
The first devices indicated for lead extraction procedures were launched by Cook in 1989. The locking stylet and Byrd Dilator Sheaths created mechanical lead extraction. Typically, all devices without a direct external energy source (i.e., lasers and radio frequency sheaths) have been classified as mechanical extraction tools. Rotational tools have taken the principles of mechanical extraction and evolved them into the newest technology available in lead extraction.
What is Rotational TLE?
Rotational transvenous lead extraction (TLE) devices have a proven track record of safety and efficacy2,3. The rotational system utilizes a “hand-powered” flexible sheath with a specialized dissection tip. The inner sheath is activated with a trigger handle allowing the user to control the amount and direction of the sheath’s rotation.
The amount of sheath rotation is directly proportional to the length of the trigger pull by the physician, while powered devices have a preset energy that is triggered upon activation.
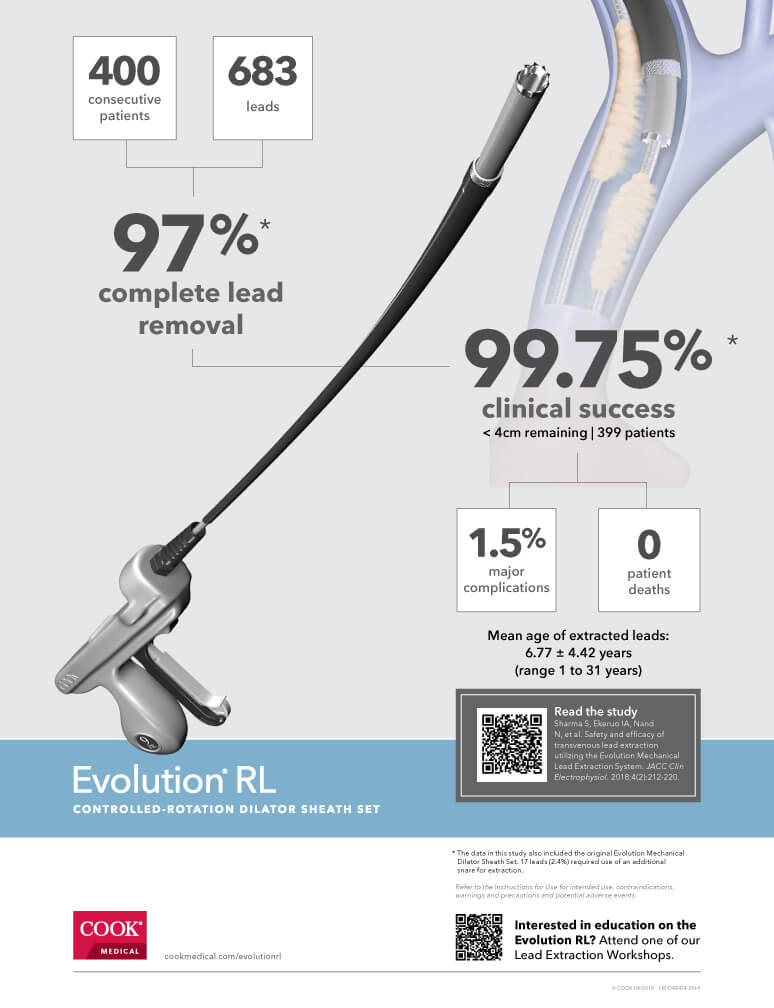
Evolution® RL Controlled-Rotation Dilator Sheath Set
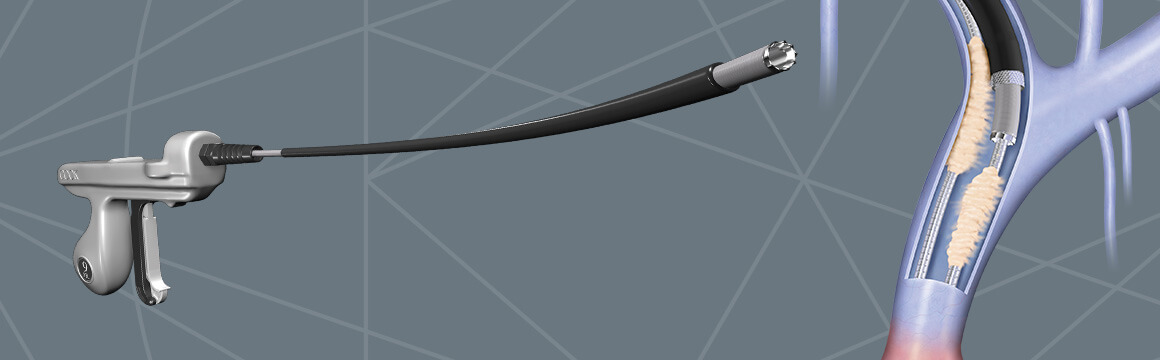
The Evolution RL is flexible enough to allow for the extraction of any lead, including in difficult vasculature. The RL gives the physician the strength and control needed when engaging with dense and calcified adhesions2,3,4,5.
The 10-sided tip allows the physician to peel the leads away from scar tissue and only engages the tissue directly surrounding the tip. The tip also allows for disrupting the tissue while rotating in either direction. The bladeless tip and bidirectional extraction mechanism have shown no occurrences of lead wrap or damage to companion leads2,4,5.
A lot has changed in lead extraction technology over the last three decades. With the input of physicians, the Evolution RL has built upon the principles of the original mechanical dilator sheaths and has been proven to be safe and effective2,3,4. Cook Medical is continuously working to provide physicians with the technology they need to keep patients safe and get them back to living.
Vista® Education and Training
To get training on the Evolution RL or any other Cook Medical devices, physicians can sign up here for our educational training courses. Renowned physicians will work shoulder-to-shoulder with you to improve outcomes. Training is typically a one- or two-day course on a specific procedure or family of procedures. Courses may include presentations, case discussions, and lectures on the indications, complications, and limitations of the procedures. Some courses may include live observations.
- Diaz C, Guo X, Whitman I, et al. Reported mortality with rotating sheaths vs laser sheaths for transvenous lead extraction. Europace. 2019;0:1-7.
- Migliore F, Testolina M, Sagone A., et al. Multicenter experience with the Evolution RL mechanical sheath for lead extraction using a stepwise approach: Safety, effectiveness, and outcome. Pacing Clin Electrophysiol. 2019;1-9.
- Sharma S, Ekeruo I, Nand N., et al. Safety and efficacy of transvenous lead extraction utilizing the Evolution mechanical lead extraction system. JACC. 2018;4(2):212-220.
- Mazzone P, Migliore F, Bertaglia E. et al. Safety and efficacy of the new bidirectional rotational Evolution® mechanical lead extraction sheath: results from a multicentre Italian registry. Europace. 2017;1-6.
- Stark CT, Steffel J, Caliskan E, et al. Clinical performance of a new bidirectional rotational mechanical lead extraction sheath. Europace. 2016;18(2):253-256.
LM-D54194-EN
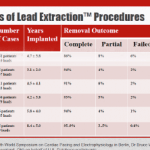
 According to a recently published study involving 400 consecutive patients and 683 leads, Cook’s Evolution system—including the Evolution RL Controlled-Rotation Dilator Sheath Set and the original Evolution Mechanical Dilator Sheath Set–has a 97% complete lead removal rate and a 99.75% clinical success rate.
According to a recently published study involving 400 consecutive patients and 683 leads, Cook’s Evolution system—including the Evolution RL Controlled-Rotation Dilator Sheath Set and the original Evolution Mechanical Dilator Sheath Set–has a 97% complete lead removal rate and a 99.75% clinical success rate.
Read the study abstract here.
Learn about and attend a Cook Vista lead extraction workshops: https://vista.cookmedical.com
LM-D48661-EN

We are looking forward to Heart Rhythm 2019 and invite you to stop by our booth (#1919) to speak with our reps and learn about Rotational TLE.
We also invite you to attend our lunchtime symposium:
Lead Extraction: Getting Patients Back to Living
Friday, May 10, 2019
12:15 – 1:15 pm
Rhythm Theater 2, Booth 2100
Chair: Raymond H.M. Schaerf, MD
Safety and efficacy with rotational TLE – Saumya Sharma, MD
Devices and techniques for improving patient outcomes – Professor Christoph Starck, MD
Mitigating SVC risk with hybrid extraction – Roger Freedman, MD
This program is not part of Heart Rhythm 2019 Official Scientific Sessions as planned by the Heart Rhythm Society Scientific Sessions Program Committee. This event is neither sponsored nor endorsed by the Heart Rhythm Society. This event does not qualify for continuing medical education (CME) credit.
Drs. Schaerf, Sharma, Starck, and Freedman are paid consultants of Cook Medical.
LM-D48598-EN
It started as a “dark art”
Lead management is important now more than ever given the growing number of devices implanted in an aging population. Lead extraction hasn’t always been at the forefront of many physicians’ skillset.
But when pacemakers were a new technology, the medical field had no standard tools or techniques for the procedure then. One pioneer in the field says removing a bad lead back then was “a dark art.”
Pacemakers were a huge step forward in caring for heart patients with abnormal heart rhythms. What no one really thought of at first was what would happen if the pacemaker or the leads attached to the heart needed to be removed or replaced.
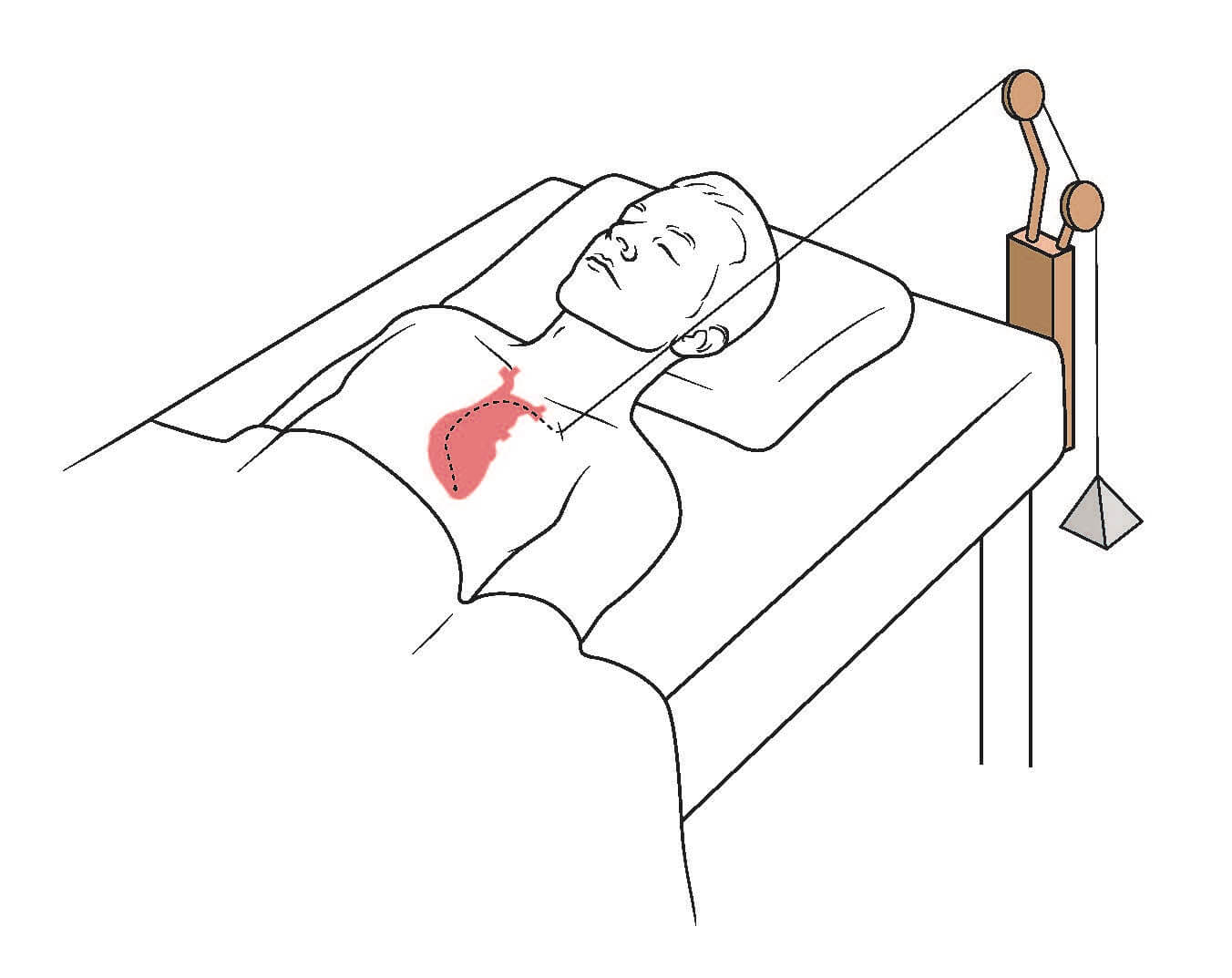
At the time, there was no standard procedure, no tools, no training available to help physicians remove leads. Physicians did the best they could. Some used direct traction—tying sutures to leads or simply pulling on the lead with their hands. Others used a weighted pulley system to gradually apply traction. Yet others approached extractions with open surgery.
Some frustrated physicians became inventors
Physicians are problem solvers at heart. Those physicians who were working with pacemakers began to see the need for removing leads, and saw the risks to the patient associated with the methods being used. Several physicians began to innovate and identified the first challenges that needed to be overcome in the procedure: Stability, binding scar tissue, and fragile materials. Some of the efforts to improve lead management include:
- Jorgen Meibom of Denmark began working on a locking stylet that locks at the tip of the lead.
- Charles Byrd of the United States was working on telescoping plastic and stainless steel dilators to separate binding scar tissue from the cardiac lead and to detach the lead from the endocardium.
- The product and engineering team from Cook Medical in the United States was working on a locking stylet and sheaths also, based on the needs they saw watching pacemaker procedures.
The locking stylet and the concept of countertraction became the core principals behind lead extraction tools.
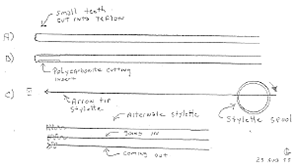
A product development sketch from 1988.
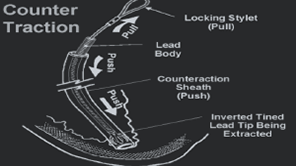
This image visually explaining counter traction was used in a training PowerPoint developed by Cook Medical.
Iteration and education was a group effort: Collaborating with the core four
A team of product managers and engineers from Cook Medical began collaborating with a core group of physicians on product development: Dr. Charles Love, Dr. Charles Byrd, Dr. Bruce Wilkoff, and Dr. Ray Schaerf. This group had the same goals of creating a safe and effective lead extraction procedure. It was a matter of overcoming technology.
Educating colleagues
This same group began working on training other physicians and raising awareness about managing the risks of lead extraction.
The Heart Rhythm Society (then called NASPE) convened a policy conference in 1997 to formalize standards, training, equipment and staffing recommendations, and indications and contraindications of lead extractions. The guidance document was originally published in April 2000. An updated version was published in 2017.
Sharing lessons
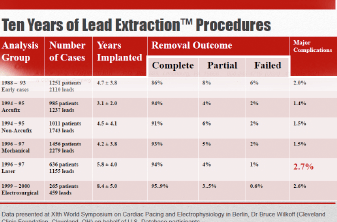
In 1989, Med Institute (the research arm of Cook Medical) began the Lead Extraction Registry to capture procedural data from 400 facilities. Data was collected for more than a decade and then shared to enhance the understanding and practice of lead extraction. This registry was the first study dedicated to lead extraction. It sparked countless other large registries and many physician-written articles continuing to the present day.
We’re never finished improving
Product innovation is always in motion. There is never a point in medical device development or procedure development where you are finished. There is always a way to make the product or procedure better. Additionally, in the case of lead extraction, the technology for pacemakers and leads is always advancing, so lead extraction technology and techniques must keep up. Each new lead creates a new challenge for extraction. From those first, simple products—a locking stylet and a telescoping sheath—the tools for lead extraction have evolved but have not strayed far from those basic principles.
Improved materials, added flexibility, increased strength, more ergonomic features, one-size-fits-all designs—these small changes can add up to big improvements over time.