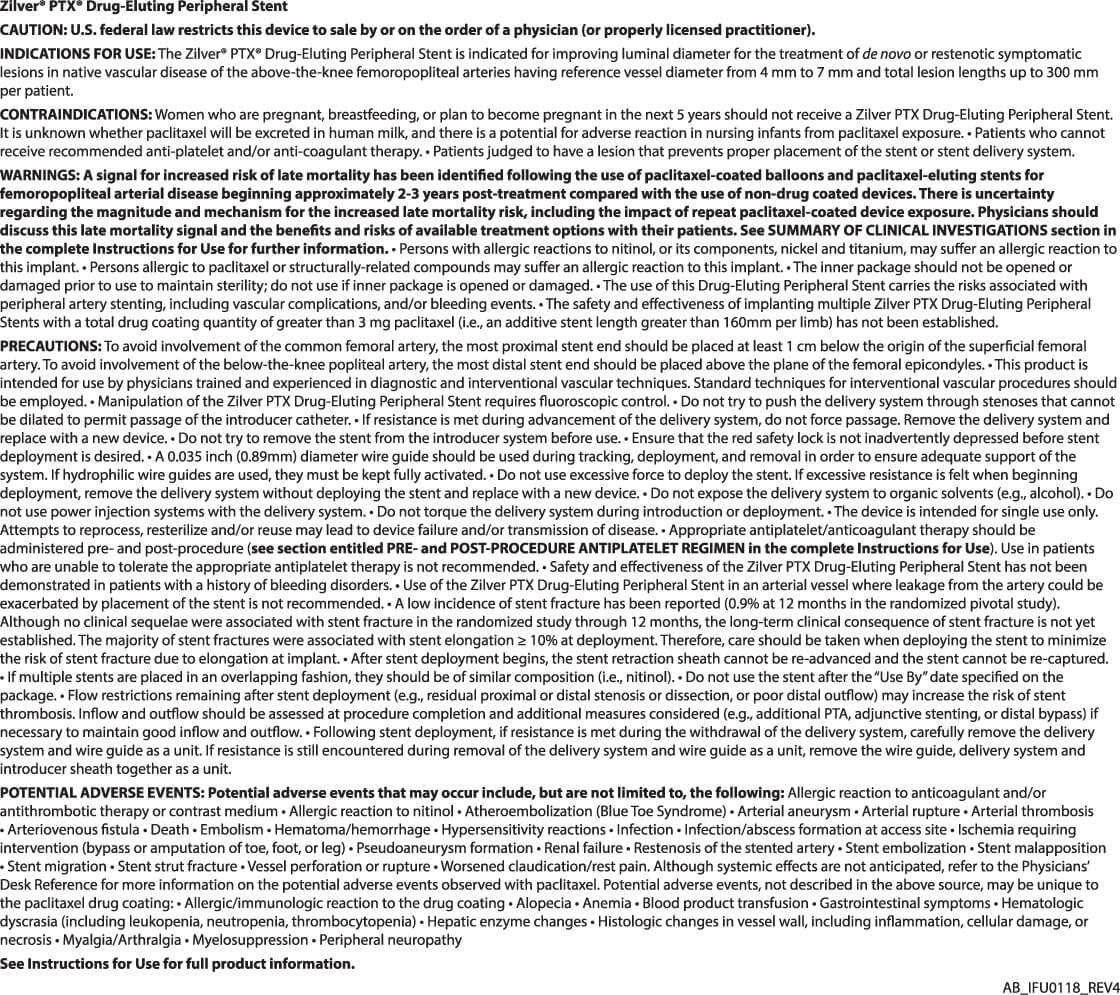
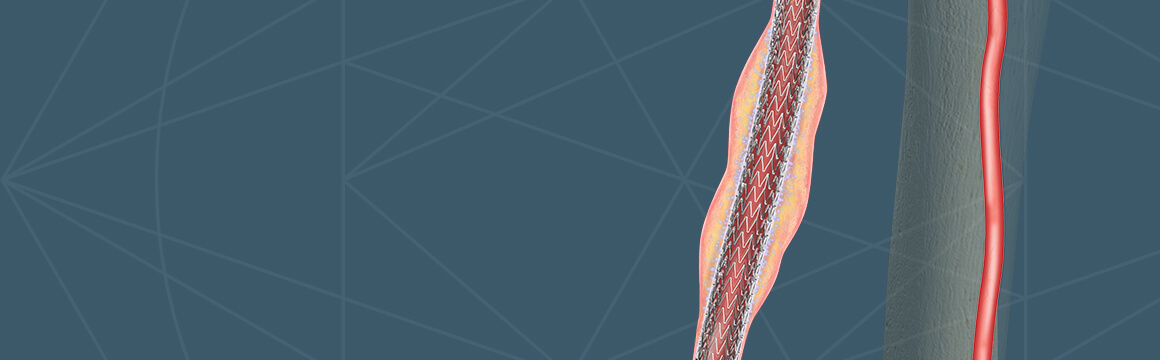
Cook’s 2nd generation CXI Support Catheter has earned its reputation as a premium technology for your procedural essentials in Peripheral Arterial Disease (PAD) cases. Cook Medical launched the new 2.6 Fr catheter on March 25, 2019, in the U.S. and Canada.
Dr. Art Lee, an interventional cardiologist at the Cardiac & Vascular Institute, and Dr. John Phillips, a cardiologist at Ohio Health, spoke with Cook Medical about their experiences using the new CXI catheter.
“It’s my go-to catheter,” said Dr. Phillips. “I use it in most of my peripheral cases.”
With new platinum-iridium marker bands, the catheter has improved visibility1 and now comes with an additional tip configuration and a new 135 cm length. This new length also provides another option for coaxial use with a 90 cm 4 Fr CXI support catheter.
According to Dr. Lee, the benefits of coaxial use are needed “wherever you need more support and has been helpful in contralateral approaches as well.”
He also remarked on the value of the added visibility of the new catheter. “Better visibility can help me reduce fluoro time.”
The CXI is one of Dr. Lee’s essential tools for PAD treatment, as well as the Approach® Hydro ST Microwire Guide, Approach® CTO Microwire Guide, Micropuncture® Pedal Introducer Access Set, and Flexor® Ansel Guiding Sheath. According to Dr. Philllips, “A good workhorse wire and support catheter can get you through most lesions.”
When it comes to retrograde access, Dr. Lee said, “I use .018 CXI catheter as my initial catheter in retrograde access and crossing, and it works exceedingly well. It is my workhorse for CLI, whether antegrade or retrograde, and many times are used in both directions.”
When asked about his ability to treat patients, Dr. Phillips said, “The catheter helps deliver consistent results, and that is what you want when you’re treating PAD/CLI day in and day out.”
Dr. Lee and Dr. Phillips are paid consultants for Cook Medical.
- Chidalek D. Technical report “Radiopacity testing of CXI catheters” (FS180470-R), Cook Research Inc., West Lafayette, Indiana; January 15, 2019.
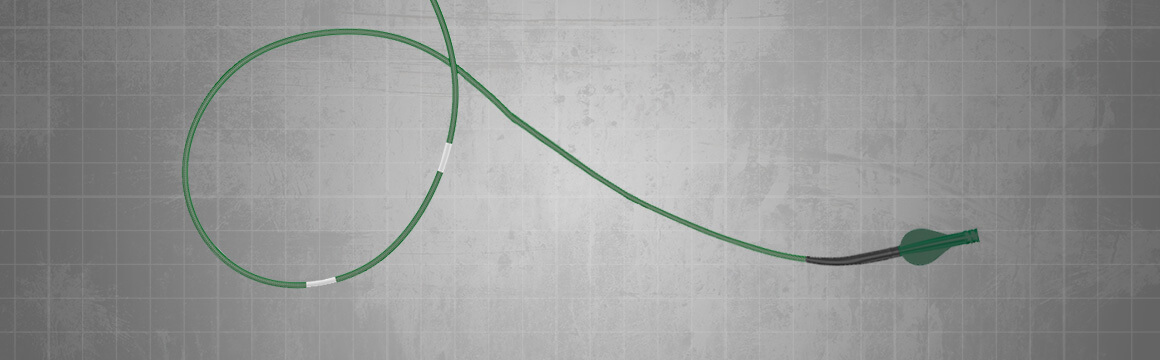
With a new 5 mm diameter stent added to the Zilver PTX arsenal, Cook Medical has expanded its offering of the broadest range of drug-eluting stent (DES) sizes available to treat peripheral arterial disease (PAD) in the superficial femoral artery (SFA).1,2
The distal SFA and proximal popliteal are often smaller diameter vessels and cannot always be treated with a DES that is sized properly to the vessel. The Zilver PTX 5 mm stent now allows physicians to treat patients who have smaller vessels with a DES.3

On Jan. 10, 2019, Dr. Robert Beasley, director of Mount Sinai’s Vascular/Interventional Radiology Lab and Evanescence Vein Center, became the first U.S. physician to use a 5 mm DES. The Miami-based interventional radiologist treated a female patient with a small SFA.
The distal SFA and proximal popliteal artery extend through the Hunter’s Canal where significant stress occurs, causing a unique challenge when treating PAD.
Dr. Beasley has been using Zilver PTX since its market release in 2012. He is currently one of the highest users of Zilver PTX in the nation. “I’ve seen significantly improved primary patency rates on follow-up imaging. This benefit is confirmed on yearly follow-up examination,” he said. “When significant restenosis occurs, it is usually manifested in short focal lesions.”
Zilver PTX is the world’s first DES used to treat PAD in the SFA and the only drug-eluting SFA stent with five-year data.4 It’s indicated for improving luminal diameter for the treatment of de novo or restenotic symptomatic lesions in native vascular disease of the above-the-knee femoropopliteal arteries having reference vessel diameter from 4 mm to 7 mm and total lesion lengths up to 300 mm per patient.1
In addition to the new 5 mm stent offering, Zilver PTX is available in 6, 7, and 8 mm diameters and lengths of 40, 60, 80, 100, 120, and 140 mm.
Dr. Beasley is a paid consultant of Cook Medical.
- Refer to the Instructions for Use (IFU0118) for a clinical data overview.
- Refer to the Instructions for Use (IFU50565157-01) for a clinical data overview.
- Cipollari S, Yokoi H, Ohki T, et al. Long-term effectiveness of the Zilver PTX drug-eluting stent for femoropopliteal peripheral artery disease in patients with no patent tibial runoff vessels—results from the Zilver PTX Japan Post-Market Surveillance Study. J Vasc Interv Radiol. 2018;29(1):9-17.
- Dake MD, Ansel GM, Jaff MR, et al. Durable clinical effectiveness with paclitaxel-eluting stents in the femoropopliteal artery: 5-year results of the Zilver PTX randomized trial. Circulation. 2016;133(15):1472-1483.
PI-D47848-EN
On March 25, Cook Medical launched the new 2.6 Fr CXI® Support Catheter with platinum-iridium marker bands. The new 2.6 Fr CXI, which is now available in the US and Canada, comes with additional tip configurations and a new 135 cm length. This new length also provides another option for coaxial use with a 90 cm 4 Fr CXI.
The CXI is used in small vessel or superselective anatomy for diagnostic and interventional procedures, including peripheral use. A popular catheter for endovascular specialists, CXI has gained name recognition as sales have continued to grow steadily since it launched eight years ago.
Platinum marker bands are already available on the 2.3 Fr platform of the CXI catheter. Because platinum-iridium bands have better visibility under fluoroscopy,1 physicians asked for the 2.6 Fr CXI to have the same visibility as the 2.3 Fr version.
“We have loyal customers who love the platinum-iridium bands on the 2.3 Fr CXI,” said Mike Williams, director of global vascular programs. “Physicians like our 2.6 Fr CXI, but asked for more visible marker bands. Because we always strive to provide physicians with the right tools for the right procedures, we listened to them and now are making CXI even better.”
CXI’s stainless steel braid provides responsive torque and pushability. A hydrophilic coating on the distal 40 cm further enhances pushability and also increases trackability. The flexible, braided catheter shaft with hydrophilic coating tracks through complex anatomy and provides support for crossing difficult lesions. Radiopaque bands at the tip and at 5, 10, and 15 cm enhance visualization and allow operators to measure vessel segments. Exterior depth markers clearly show progression into the sheath.
The 2.3 Fr and 2.6 Fr sizes can fit coaxially in the 4.0 Fr size to increase the amount of support. The smaller sizes can also pass through the Micropuncture® Pedal Access Set and can fit in any catheter that has an .035 inch lumen.
For more information, contact your local sales representative. To view a complete parts listing, please click here.
-
Chidalek D. Radiopacity testing of CXI catheters: Generation 1 and Generation 2 (2019); FS180470-R.
PI-D47842-EN
On Dec. 6, Dr. Konstantinos Katsanos and his coauthors created tremendous controversy when they published a meta-analysis on paclitaxel-coated balloons and stents in the Journal of the American Heart Association.
Using data from 28 randomized controlled trials (RCT), the authors determined that patients suffering from peripheral arterial disease (PAD) in the superficial femoral artery (SFA) have a higher risk of mortality at two- and five-year endpoints if treated with paclitaxel-coated devices compared to treatment with uncoated devices.
The results of the meta-analysis are critically important to physicians because drug-eluting stents and balloons are considered by many to be the gold standard for endovascular treatment1,2,3 of PAD in the SFA.
Physicians from around the world who have participated in many of these RCTs recently spoke about the authors’ conclusions at LINC in Leipzig, Germany, and most recently at ISET in Hollywood, Fla. The majority of presenters agreed that the meta-analysis was important in its focus on patient safety but that more information was needed to prove causality.
 Dr. Gary Ansel, an interventional cardiologist and System Medical Chief for Vascular Services at OhioHealth, participated in the opening townhall session at ISET discussing what practitioners should do in light of the information released in the meta-analysis. The panelists were also asked if there is enough concern to alter current standards of practice.
Dr. Gary Ansel, an interventional cardiologist and System Medical Chief for Vascular Services at OhioHealth, participated in the opening townhall session at ISET discussing what practitioners should do in light of the information released in the meta-analysis. The panelists were also asked if there is enough concern to alter current standards of practice.
A live poll during the session showed 93% of the audience were surprised by the article. “This meta-analysis came out of nowhere,” said Dr. Ansel, a global co-investigator in the Zilver® PTX® RCT. “It’s unfortunate that, because of the way it was released, the article created a frenzy. A meta-analysis is designed for hypothesis generation and, unless there is patient-level data, it is not designed to prove causality.”
According to Dr. Ansel, there are a number of factors that confounds the findings of the meta-analysis. “For example, physicians in RCTs are not blinded, so they might have used higher doses of statins or platelets in the control arm,” he said. “This was not part of our trial design. Biases could have occurred.”
In addition, the meta-analysis did not look at patient-level data. “Based on the information reported, the connection between mortality rates and use of paclitaxel devices is not conclusive,” Dr. Ansel said. “With regard to Zilver PTX, results from previous patient-level analyses demonstrate no causality between exposure to paclitaxel and mortality through five years.”
He noted that the authors claimed that Zilver PTX has one of the highest dose densities of all paclitaxel-coated devices on the market. “This is misleading because it’s a stent. Only 10 to 20 percent of the surface is coated compared to paclitaxel-coated balloons,” he said. “Physicians need to be much more accurate and balanced when they look at things scientifically. If you look at Zilver PTX, you should know it’s actually the lowest-level drug dose device included in this meta-analysis. We then must also look at other potential variables than paclitaxel.” Besides dosage, variables might include cause of death, prescription of other medications, and co-morbidities.
While the article has received pushback, Dr. Ansel stressed that physicians should not make light of the meta-analysis results just because they don’t agree with its design. “This was a peer-reviewed article published in a reputable journal,” he said. “It’s an analytically reasonable article. We might not agree on all the variables, but it is still accepted methodology.”
To help provide objective analysis on the issue, the VIVA Vascular Leaders Forum (VLF) will gather in Washington, DC, from March 1-2 alongside an international community of physicians including oncologists, regulatory scientists, an independent statistician, as well as patients to discuss industry data analyses.
The VLF will bring together people unrelated to industry to help frame the discussions. “VIVA is only helping to facilitate the meeting and will let the experts without device industry disclosures lead the discussion,” said Dr. Ansel, a member of the VIVA board of directors. “We are trying to make sure that we are doing this in a very responsible fashion. We want everyone’s input on this.”
Dr. Ansel said he looks forward to the VLF analysis. “This will be a great opportunity to examine further analysis and guidance going forward,” he said. “We all take patient safety very seriously. But we shouldn’t get rid of therapeutic devices that have shown excellent long-term results until we have more data.”
Dr. Ansel is a paid consultant for Cook Medical.
- Dake MD, Ansel GM, Jaff MR, et al. Durable clinical effectiveness with paclitaxel-eluting stents in the femoropopliteal artery: 5-year results of the Zilver PTX randomized trial. Circulation. 2016;133(15):1472-1483.
- Rosenfield K, Jaff M, White C, et al. Trial of a paclitaxel-coated balloon for femoropopliteal artery disease. N Engl J Med. 2015; 373:145-153.
- Schneider P, Laird J, Tepe G, et al. Treatment Effect of Drug-Coated Balloons Is Durable to 3 Years in the Femoropopliteal Arteries Long-Term Results of the IN.PACT SFA Randomized Trial. Circ Cardiovasc Interv. 2018;11.
PI-D47519-EN